
Views: 210
– Proff. Giancarlo Isaia and Enzo Medico, from the University of Turin, on the possible preventive and therapeutic role of vitamin D in the treatment of the COVID-19 pandemic
Condensed by Hernan Valenzuela at Minapim: The clinical and epidemiological presentation of the Coronavirus pandemic is certainly very anomalous and, in search of possible contributing factors or specific risk factors, Prof. Giancarlo Isaia, Professor of Geriatrics and President of the Academy of Medicine of Turin, and Prof. Enzo Medico, a full professor of histology at the University of Turin, also following the recent recommendations of the British Dietetic Association, deepened the role that the lack of vitamin D could play, which in Italy affects a large part of the population, especially the elderly.
Thus, some data emerged that, summarized in a document, have already been submitted to members of the Academy of Medicine of Turin, were considered very interesting. In it, the authors suggest to doctors, in association with the well-known general preventive measures, to guarantee adequate levels of vitamin D in the population, but above all in those already infected, in their family members, in the health team, in frail elderly people, guests in care homes , in people under a cloister and in all those who, for various reasons, are not adequately exposed to sunlight.
In addition, administration of the active form of vitamin D, calcitriol, intravenously in patients with COVID-19 and with particularly impaired respiratory function can also be considered.
These indications are derived from numerous scientific evidences that showed:
1.a) An active role of vitamin D in the modulation of the immune system
2.b) The frequent association of hypovitaminosis D with numerous chronic diseases that can reduce life expectancy in the elderly, especially in the case of COVID-19 infection.
3.c) Effect of vitamin D in reducing the risk of respiratory infections of viral origin, including those caused by coronavirus.
4.d) The ability of vitamin D to neutralize lung damage caused by hyper-inflammation.
In addition, the first preliminary data currently collected in Turin indicate that patients with COVID-19 have a very high prevalence of hypovitaminosis D. Compensation for this wide vitamin deficiency can be achieved mainly by exposure to sunlight as much as possible, balconies and terraces, eating foods rich in vitamin D and, under medical supervision, taking specific pharmaceutical preparations.
The study presented:
With reference to useful measures to combat the effects of the Coronavirus pandemic, we believe it is appropriate to draw attention to an aspect of prevention, less known to the general public, Hypovitaminosis D whose compensation, in association with the well-known general preventive measures, could help to overcome this difficult moment.
Based on numerous scientific evidences and epidemiological considerations, it seems that obtaining adequate plasma levels of vitamin D is necessary, above all, to avoid numerous chronic pathologies that can reduce life expectancy in the elderly, but also to determine greater resistance to COVID-19 infection which, although with less scientific evidence, can be considered probable.
This compensation can be achieved mainly with proper exposure to sunlight and then eating foods rich in vitamin D (Figure 1 shows the ten foods in which it is most present) and, finally, with the intake of specific pharmaceutical preparations, always under medical supervision.
This recommendation is useful for the general population, but it is particularly significant for individuals already infected, their family members, health personnel, frail elderly people, guests in nursing homes, pregnant women, people on the premises and all those who, for various reasons , are not properly exposed to sunlight. In addition, the acute administration of calcitriol by e.v. in COVID-19 patients with particularly impaired respiratory function
Presence of Vitamin D
– A 45 µg herring – A 19.5 µg horse mackerel – A 16.5 µg sea bass fillet
– A dozen anchovies 16.5 µg – A small horse mackerel 4.4 µg
– Half dish of chiodini mushrooms 4.2µg – Red mullet 2 µg
– A handful of dried 1.1 µg shitake mushrooms – Egg 0.9 µg
– A small 0.5µg tofu –
Recommended daily intake of vitamin D for the adult population 15µg
Even if there is no complete agreement between different scientific societies, we can consider them acceptable in the general population above 20 ng / ml, while in the elderly it would be appropriate to reach at least 30 ng / ml. Vitamin D can be synthesized by the skin, due to the effect of ultraviolet radiation emitted by sunlight, which determine the conversion of the 7 dehydrocholesterol in Colecalciferol, or may be found with food.
Once produced from the skin or taken with food, cholecalciferol yes accumulates in the adipose tissue to be gradually released and meets two successive hydroxylations, the first liver (25 OHD) and the second in the kidney, with production of its active form (1 -25 OH2 D3 or calcitriol) which then, by binding to specific receptors, acts on different tissues with a hormonal-like mechanism. During winter, cholecalciferol levels are significantly reduced, due to less solar radiation and the depletion of reserves accumulated during the summer: for this reason, in February / March there is a greater risk of scarcity.
Synthesis of vitamin D3 from exposure to the sun and food. By Allison Clark and Núria Mach
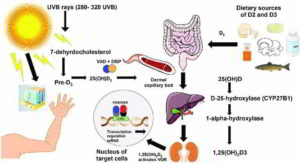
Vitamin D is synthesized from exposure to the sun or consumption of foods rich in vitamin D. The sun’s ultraviolet B rays at frequencies between 280 and 320 reach the skin, where 7-dehydrocholesterol is converted into pre-vitamin D3 and then isomerized in vitamin D3. or cholecalciferol.
The vitamin D-binding protein facilitates the entry of vitamin D3 into the dermal capillary bed. To the right of the figure, vitamin D2 ingested (ergocalciferol) from food or supplements is incorporated into the chylomicrons, which enter the lymphatic system and the blood.
Once in the bloodstream, vitamin D2 and vitamin D3 travel to the liver, where the cytochrome P450 enzyme hydroxylates the two forms of the vitamin to 25 (OH) D3. Then, CYP27B1 hydroxyl plus 25 (OH) D3 in the active form of vitamin [1.25 (OH) 2D3] in the kidneys.
Unlike D2 or other metabolites of vitamin D, vitamin D3 is the active form of vitamin D that binds to the vitamin D receptor (VDR), located in about 30 different tissues. Activated VDR binds to vitamin D-responsive elements (VDREs) to form a heterodimer, which can directly or indirectly regulate the expression of ~ 3% of mouse and human genomes.
Sources: Giancarlo Isaia and Enzo Medico, University of Turin Frontiers in Immunology Allison Clark and Núria Mach
Related article: Reducing the risk of virus infection including COVID